
Choking
Table of Contents

What is erotic choking?
Similar to the concept of a chokehold in martial arts, but used for the sake of arousal and pleasure, an erotic choke is a grappling hold that restricts either air (asphyxiation or suffocation) or blood (strangulation) from passing through one's neck. The restriction may involve a combination of both asphyxiation and strangling, depending on the points of pressure.
Usually performed using just bare hands (which is generally safer), it can also be performed through the use of other body parts (such as the thighs, discussed on the smothering section) or even tools (such as ropes). The risk for severe and irreversible damage increases exponentially with the use of stronger means like thighs or ropes, so using just the hands is advisable in most cases.
The name "erotic asphyxiation", sometimes used as a synonym for choking, can be misleading, belittling the vascular repercussions of neck compression (the blood flow restriction). Although it is possible to cause exclusively airway obstruction (asphyxiation) or exclusively blood flow obstruction (strangling), there is more often than not an association of both in most forms of neck compression. For this reason the term "erotic choking" is preferable, unless you are talking about a practice of exclusive breath play (see breath play).
Is erotic choking safe?
It depends entirely on the circumstance. Erotic choking can range from quite safe to extremely dangerous, depending on what exactly is done. It's reasonable to say this is an advanced kink, meaning there are many prerequisites one must know in order to execute it as safely as possible. Considering the vulnerability of the neck structures, however, there is always some degree of risk, making the RACK (Risk Aware Consensual Kink) acronym a paramount parameter for this kink.
Although there is a lack of peer-reviewed data regarding erotic choking specifically (partially because it's still a taboo for many), there is much to be learned from the knowledge steeming from chokeholds in martial arts, which have existed for a long time and do have some degree of formal research behind them in regards to safety, short and long-term consequences. Furthermore, there is also much to be said from a medical perspective regarding neck trauma. Teachings based on personal, anecdotal experience coming from lay practitioners should be taken carefully.
Erotic choke roleplaying
Pretending to choke someone is the safest way of practicing this kink. For some people it might not be arousing enough, but it's a possibility to keep in mind, especially for beginners in the practice. It may sound lackluster, but give it a try: a hand positioned around one's neck, with a firm grasp (but without applying any pressure), creating the threat of a choke, can produce good (and safe) results in terms of arousal.
That being said, let's go over what you should know about neck anatomy to both minimize risks and be aware of what can go wrong when actually practicing erotic choking.
Midline neck structures: airway obstruction (asphyxiation)
Functional details about breathing, asphyxiation, hypoxemia, hypoxia and hypercapnia are discussed here.
The human airway goes through the center of the neck (larynx and trachea), as shown in the picture below. There are no gas exchanges here (hence why it's called an anatomical dead space), meaning this is purely a highway for the atmospheric air to reach the lungs.
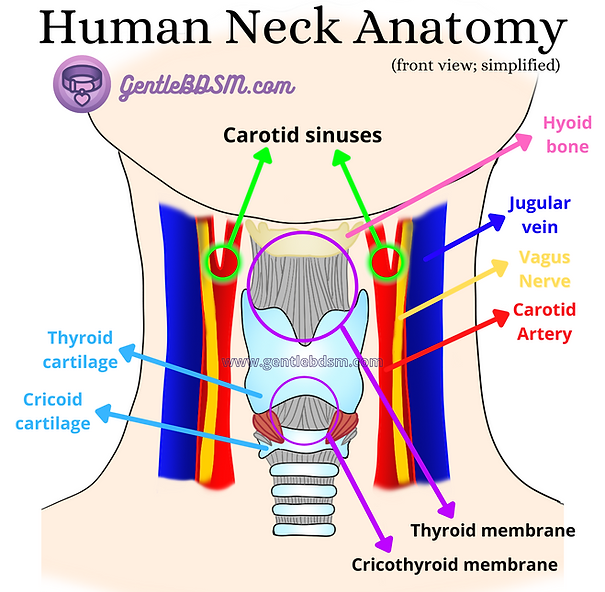
Picture 1 - Anatomical structures of the neck (simplified)
The upper portion (roughly the upper half), called the larynx, displays a number of discernible anatomical features. The most relevant ones for this subject are the thyroid cartilage and the cricoid cartilage. Both are rigid ring-like structures identifiable through palpation of the neck's midline. The thyroid cartilage, which is the upper one, has a prominence called Adam's apple (or laryngeal prominence), which is often visible, especially in males and AMAB (assigned male at birth, assuming it was not surgically removed).
The thyroid cartilage's prominence is an extremely important point of reference for this practice. Right above it is the thyroid membrane, while below it is the cricothyroid membrane. The thyroid membrane connects the thyroid cartilage to a small ring-like bone below the chin, called hyoid bone, which may or may not be palpable. The cricothyroid membrane, as its name suggests, connects the thyroid cartilage to the cricoid cartilage below, which is often palpable as well. These two membranes are the weakest spots along the neck's airway, making them critical spots to be aware of.
The bottom portion (below the cricoid cartilage), called the trachea (also known as "windpipe"), is a cartilaginous tube that connects the larynx above to the bronchi of the lungs below it. Its cartilaginous covering means this is not a compressible structure, i.e. you do not easily "close" it through external compression - you merely push it backwards, since the structure behind it (the esophagus) is much softer. The trachea is quite resistant, albeit flexible. It's like a hard rubber pipe, not a soft tube. Understanding this is essential, because there is a lot of fearmongering surrounding these concepts, as if one could easily obstruct the lumen (the open space inside) of the trachea through external compression. Actual trauma to this structure (seen here) generally requires higher amounts of biomechanical energy (such as from a car crash or a gun wound). Other structures adjacent to the trachea, like the vagus nerve, carotid arteries and jugular veins, are all more vulnerable and susceptible to damage upon compression (seen here). The same concept applies to compressions of the thyroid and cricoid cartilages, which will most likely push the larynx back, instead of actually collapsing it.
Cartilages such as the ones found around the larynx and the trachea are extremely resistent, considering their purpose is to protect the airways. Similarly to bones, they can also break or suffer fractures (seen here and here), but it is extremely unlikely to have such an outcome through manual compression of the neck. This means that midline compressions of the neck, assuming they are not centered at the membranes mentioned above, should be reasonably safe. It won't easily lead to asphyxiation, contrary to popular belief. In order to cause asphyxiation, all the structures around the airways of the neck must be compressed against each other with a much higher force, meaning it is very hard to cause pure asphyxiation without strangulation, except for direct compression of either the thyroid of cricothryroid membranes.
Disclaimer about autoerotic asphyxiation (AEA): trying to perform breath play by yourself is an extremely risky and life-threatening activity. We do not recommend trying it under any circumstances, as the risk of accidental death is high and there's not much to be done if something goes wrong, considering you'll be alone.
Lateral neck structures: bloodflow obstruction (strangling)
Laterally (i.e. externally) to the midline airway structures, major blood vessels are found, namely the carotid arteries and jugular veins. The carotid arteries take oxygenated blood from the heart (after passing through the lungs) into the head structures, including the brain, while the jugular veins extract deoxygenated blood back from these same structures.
As is often the case with blood vessels, the (jugular) veins have much weaker walls than the (carotid) arteries, meaning they are more easily collapsed through compression. As such, during a choking act, blood flow from the brain slows down first, rather than blood supply to the brain. This, however, dams up the deoxygenated blood within the head, slowing down its flow. Since the carotid arteries are subject to the same compression, they are not able to acommodate any changes the heart may undertake in order to re-establish proper blood flow to the head structures, especially the brain, such as increasing the provided flow. Saying neck compression causes a "decrease in blood flow to the brain" is, therefore, a simplified misconception. It actually traps deoxygenated blood within the entire head. As such, it technically increases the amount of blood in the brain, but it's deoxygenated blood, with a higher concentration of CO2 (carbon dioxide), since the tissues keep extracting O2 and exchanging it for CO2, even though the oxygenated blood supply is not being replenished fast enough.
The brain perceives this increase in deoxygenated blood as asphyxiation, even though it might technically not be. There is, however, a true hypoxia to the brain tissue, which may lead to irreversible damage. See breath play for more information about the symptons of brain hypoxia.
Carotid sinus reflex, atherosclerosis and stroke
Compressing the carotid arteries on the neck poses threats of its own. Some lay people think that is because blood supply to the brain is mechanically restricted, but this is not the case - as mentioned priorly, the carotid arteries are not so easily obstructed by external compression. Obstruction of the jugular veins is what ultimately leads to an increase in deoxygenated blood in the brain.
So what is the issue of compressing the carotid arteries? They can be divided in two groups: causing a carotid sinus reflex (which then reduces bloodflow to the brain due to a severe, sudden hypotension) and dislodging an atherosclerosis plaque (which may lead to a stroke).
The carotid sinus, shown in the picture below, contains baroreceptors which monitor blood pressure. Mechanically compressing them creates the false reading that arterial pressure has suddenly risen, which triggers a systemic reflex akin to the so-called vasovagal episode by inducing (supposedly compensatory) hypotension. This may lead to a syncope (loss of consciousness) due to insufficient blood supply to the brain (check back Picture 1).
If the person being strangled has carotid atherosclerosis (which is extremely common in people above 40 years), the mechanical trauma may rupture an existing plaque and either lead to local obstruction of the carotid artery due to the formation of a blood clot (causing a massive, often lethal stroke), or a smaller embolic stroke by releasing the dislodged plaque piece into smaller vessels of the cerebral circulation (which may still cause irreversible brain damage).
That is not to say younger people are free of risks. Albeit rare, fibromuscular dysplasia (FMD) is a systemic vascular disease that may cause carotid artery stenosis in younger patients, especially women.
Sources for additional reading
-
Pathophysiology and Medical Treatment of Carotid Artery Stenosis
-
Evaluation and Management of Atherosclerotic Carotid Stenosis: [1], [2]
-
Carotid Plaque With High-Risk Features in Embolic Stroke of Undetermined Source
In case of a partner collapse, it might be difficult for a lay person to differentiate a syncope from a cardiac arrest. It is no longer recommended for a non-healthcare professional to try checking for breathing nor pulse, since multiple studies (see sources below) have shown how unreliable that can be. A lay person should no longer try to execute mouth-to-mouth breathing, either. The "hands-only CPR" approach (only chest compressions) is now enforced for this case, as explained below.
Because of this, the conduct in case of a partner collapse should vary, depending on your education in terms of healthcare:
- Physicians, nurses and paramedics should have their Advanced Cardiac Life Support (ACLS) training updated every 2 years to apply it properly
- Other healthcare professionals should have their Basic Life Support (BLS) training updated every 2 years to apply it properly
- Lay people (i.e. non-healthcare professionals) should learn the current "hands-only CPR" approach, according to the 2020 CPR guidelines from ILCOR*.
-
Hands-only cardiopulmonary resuscitation (HO-CPR) explanation by the American Heart Association (AHA), including a quick video guide
Always know by heart or have it on your phone contacts the emergency number of the country you are in.
* ILCOR (International Liaison Committee on Resuscitation):
- American Heart Association (AHA)
- InterAmerican Heart Foundation
- European Resuscitation Council
- Heart and Stroke Foundation of Canada
- Australian and New Zealand Committee on Resuscitation
- Resuscitation Councils of Southern Africa
Sources for additional reading about lay people and CPR: [1], [2], [3]. [4], [5]. [6], [7]